
Last updated: May 17, 2026
Quick Answer: Using vitamins supplements as a treatment means taking specific micronutrients to address deficiencies, support recovery, or manage certain health conditions under medical guidance. The evidence ranges from strong (Vitamin D for bone health, B12 for deficiency-related anemia) to weak (high-dose antioxidants for cancer prevention). Supplements work best when they correct a documented deficiency or fill a genuine dietary gap — not as a blanket substitute for medical care.
Key Takeaways
- 🧪 Supplements treat deficiencies effectively — Vitamin D, B12, iron, and folate have strong clinical backing when a deficiency is confirmed by blood testing.
- ⚠️ More is not always better — Fat-soluble vitamins (A, D, E, K) can accumulate to toxic levels if over-supplemented.
- 🩺 Medical supervision matters — Some supplements interact with prescription medications (e.g., Vitamin K and warfarin, St. John’s Wort and antidepressants).
- 📊 Quality varies widely — Third-party certifications (USP, NSF International, ConsumerLab) help verify that a product contains what the label claims.
- 🌍 Deficiencies are common globally — The World Health Organization estimates that micronutrient deficiencies affect over 2 billion people worldwide (WHO, 2023).
- 🔬 Therapeutic doses differ from dietary doses — A treatment dose prescribed by a clinician can be many times higher than the standard Recommended Dietary Allowance (RDA).
- 💊 Food-first is still the gold standard — Supplements fill gaps; they rarely replicate the full benefit of a nutrient-rich diet.
- 🚫 Not all claims are FDA-approved — In the United States, dietary supplements are regulated as foods, not drugs, meaning manufacturers cannot legally claim they treat or cure diseases.
What Does “Using Vitamins Supplements As A Treatment” Actually Mean?
Using vitamins supplements as a treatment refers to the deliberate, clinically informed use of micronutrient supplements to correct a deficiency, support a disease-management plan, or reduce the risk of a specific health outcome. This is distinct from casual supplementation for general wellness.
There are three broad categories:
- Corrective treatment — Restoring a nutrient to normal levels (e.g., Vitamin D injections for severe deficiency, B12 shots for pernicious anemia).
- Adjunct therapy — Supporting conventional medical treatment (e.g., folate supplementation during pregnancy to prevent neural tube defects).
- Preventive use — Reducing the risk of a future condition (e.g., calcium and Vitamin D for osteoporosis prevention in postmenopausal women).
Common mistake: Treating supplements as interchangeable with pharmaceuticals. Supplements support physiology; they rarely replace drug therapy for acute or serious conditions.
Which Vitamins and Supplements Have Strong Treatment Evidence?
The strongest evidence supports supplement use when a specific deficiency is confirmed and the supplement directly addresses that gap. Below is a practical overview:
| Supplement | Condition Treated | Evidence Level | Notes |
|---|---|---|---|
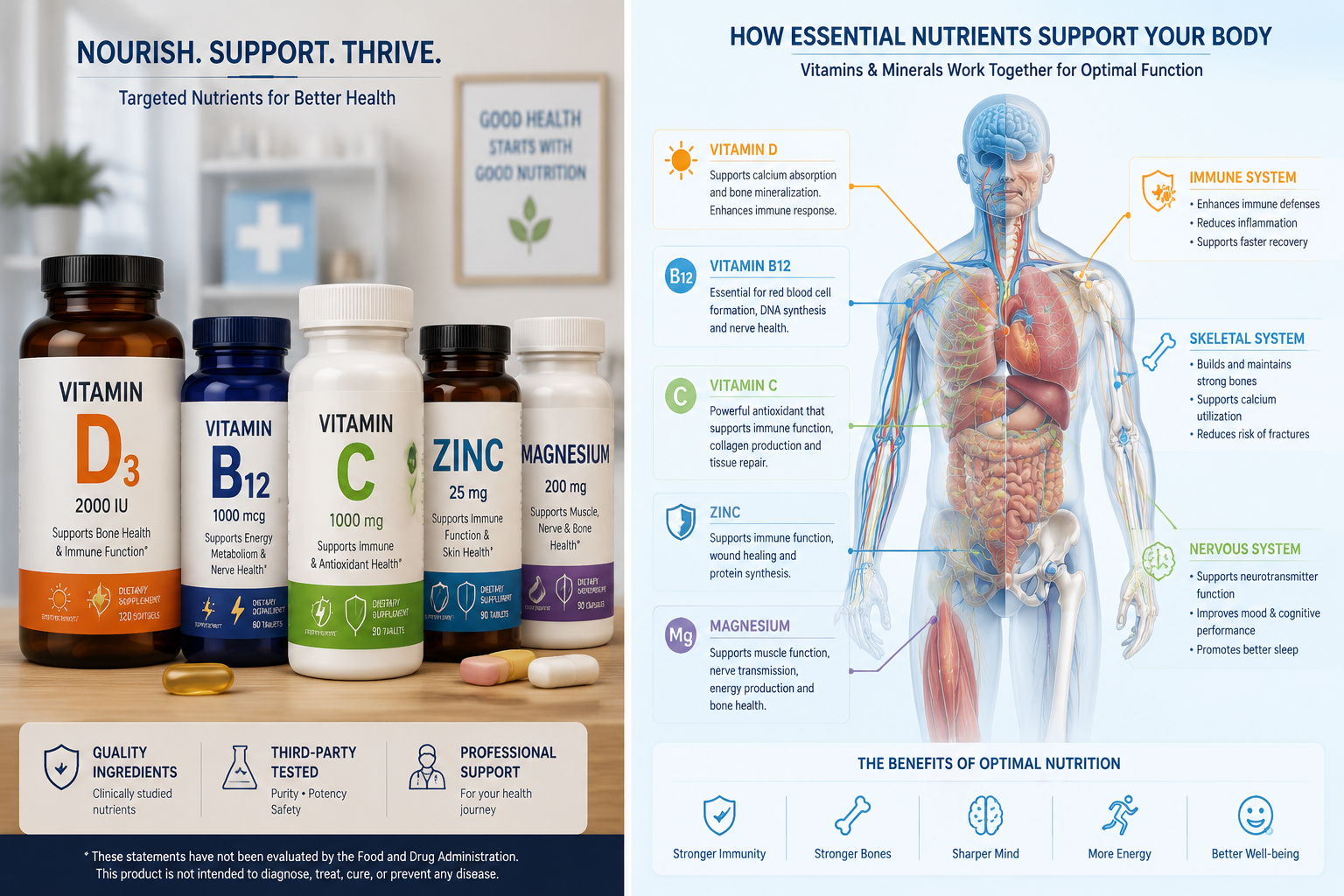
| Vitamin D | Deficiency, bone loss, rickets | Strong | Blood test (25-OH-D) recommended first |
| Vitamin B12 | Deficiency anemia, neuropathy | Strong | Especially in vegans, older adults |
| Folate (B9) | Neural tube defect prevention | Strong | Critical in early pregnancy |
| Iron | Iron-deficiency anemia | Strong | Confirm with ferritin test; excess is harmful |
| Vitamin C | Scurvy, wound healing support | Strong | High doses may cause GI distress |
| Zinc | Immune support, wound healing | Moderate | Short-term use; long-term excess depletes copper |
| Omega-3 (fish oil) | High triglycerides | Moderate-Strong | FDA-approved prescription form (Vascepa) exists |
| Magnesium | Deficiency, migraine prevention | Moderate | Often depleted by medications like PPIs |
| Vitamin A | Night blindness, deficiency | Strong | Toxic in excess; avoid high doses in pregnancy |
| Vitamin K | Bone health, clotting support | Moderate | Interacts with blood thinners |
Choose corrective supplementation if: A blood test confirms a deficiency and dietary changes alone are insufficient or impractical.
Avoid self-prescribing high doses if: You take prescription medications, are pregnant, have kidney disease, or have a condition affecting nutrient absorption.
How Are Therapeutic Doses Different from Standard RDAs?
Therapeutic doses used in using vitamins supplements as a treatment can far exceed standard dietary recommendations. The RDA is designed to meet the needs of healthy people — not to correct a clinical deficiency or achieve a pharmacological effect.
For example:
- The RDA for Vitamin D is 600–800 IU per day for most adults (National Institutes of Health, 2023).
- A physician treating documented Vitamin D deficiency may prescribe 50,000 IU weekly for 8–12 weeks.
This gap between dietary and therapeutic dosing is why self-diagnosis and self-treatment carry real risks. Fat-soluble vitamins (A, D, E, K) are stored in body fat and liver tissue, so excessive intake builds up over time and can cause toxicity.
Water-soluble vitamins (C, B-complex) are generally safer at higher doses because excess is excreted in urine — but even these have upper limits. High-dose Vitamin B6 (above 100 mg/day long-term) has been linked to peripheral neuropathy (NIH Office of Dietary Supplements, 2023).
Who Benefits Most from Using Vitamins Supplements As A Treatment?
Certain groups face higher deficiency risks and are most likely to benefit from targeted supplementation:
- Older adults — Reduced stomach acid limits B12 absorption; reduced sun exposure lowers Vitamin D synthesis.
- Vegans and vegetarians — At risk for B12, iron, zinc, omega-3, and Vitamin D deficiencies.
- Pregnant and breastfeeding women — Increased demand for folate, iron, iodine, and DHA.
- People with malabsorption conditions — Crohn’s disease, celiac disease, and bariatric surgery patients often need supplementation regardless of diet quality.
- People on certain medications — Metformin depletes B12; proton pump inhibitors reduce magnesium and B12 absorption; statins may lower CoQ10 levels.
- Those with limited sun exposure — Vitamin D deficiency is especially common in northern latitudes and among people who work indoors.
Edge case: Even people eating a varied diet can develop deficiencies if absorption is impaired. A “healthy diet” does not guarantee adequate nutrient status — blood testing is the only reliable way to confirm.
What Are the Risks and Limitations of Supplement-Based Treatment?
Using vitamins supplements as a treatment is not risk-free. The most common problems fall into three categories:
1. Toxicity from excess intake
- Vitamin A toxicity can cause liver damage, bone loss, and birth defects.
- Iron overload (hemochromatosis) can damage organs in people with a genetic predisposition.
- Excess Vitamin D raises blood calcium, potentially causing kidney stones.
2. Drug-nutrient interactions
- Vitamin K reduces the effectiveness of warfarin (a blood thinner).
- Calcium supplements can reduce absorption of thyroid medication (levothyroxine) if taken together.
- High-dose Vitamin E may increase bleeding risk in people taking aspirin or anticoagulants.
3. Product quality issues
- A 2023 ConsumerLab analysis found that a significant percentage of tested supplements contained either more or less of the stated ingredient than the label claimed.
- Contamination with heavy metals or undisclosed pharmaceutical compounds has been documented in products marketed for weight loss and sports performance.
Practical safeguard: Look for supplements certified by USP (United States Pharmacopeia), NSF International, or ConsumerLab. These third-party programs test for label accuracy and contaminant levels.
How to Use Vitamins and Supplements Safely as a Treatment
A structured approach reduces risk and improves outcomes when using vitamins supplements as a treatment:
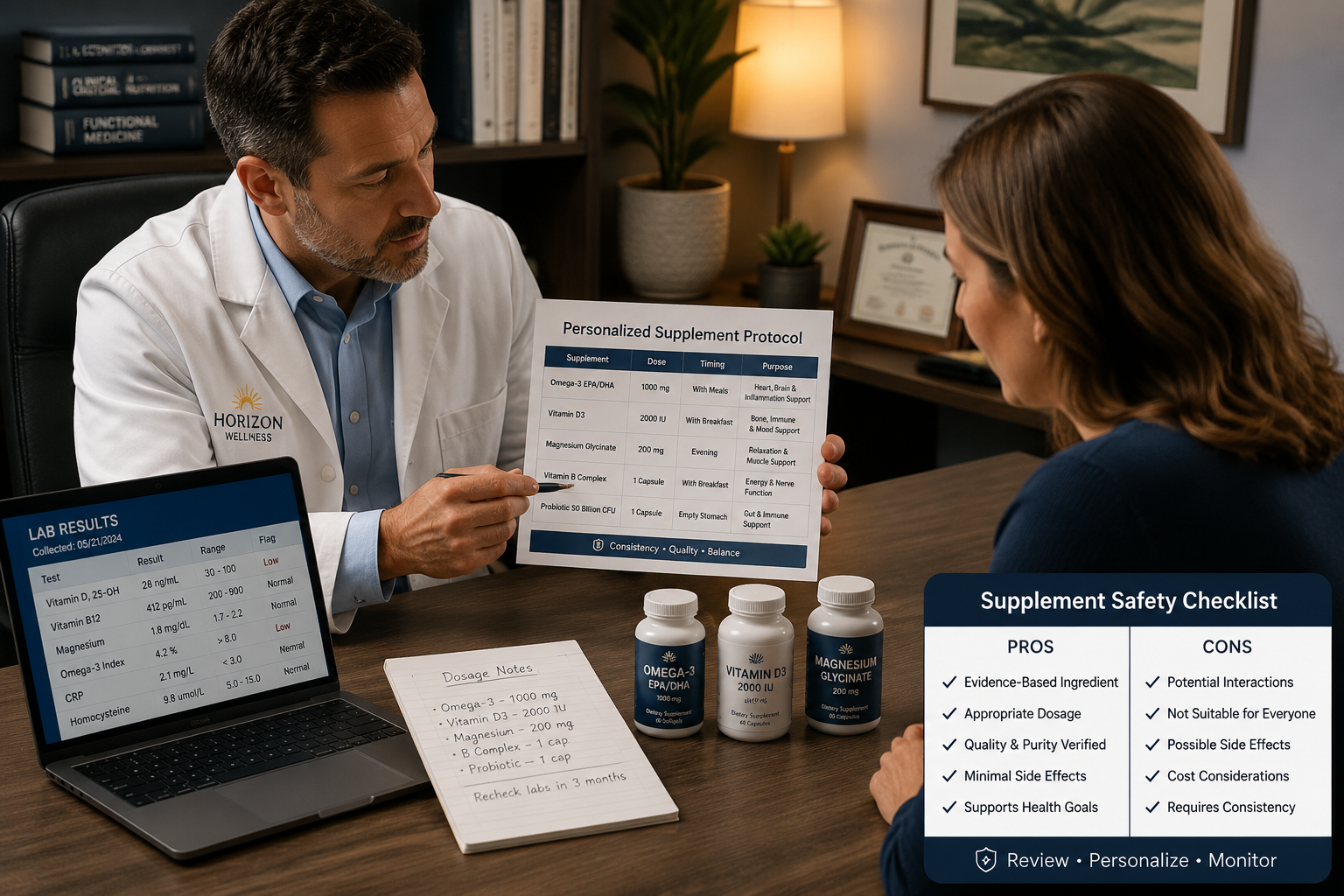
- Get tested first. Request a blood panel that includes 25-OH Vitamin D, B12, ferritin (iron stores), folate, and a complete metabolic panel. This establishes a baseline.
- Identify the deficiency or gap. Work with a healthcare provider to confirm whether a deficiency exists and whether diet alone can correct it.
- Choose the right form. Bioavailability varies by form. For example, magnesium glycinate is better absorbed than magnesium oxide; methylcobalamin is preferred over cyanocobalamin for B12 in some individuals.
- Start at the recommended therapeutic dose. Do not assume more is better. Follow clinician guidance or established upper tolerable intake levels (ULs) from the NIH.
- Check for interactions. Use a pharmacist or a drug-nutrient interaction checker before combining supplements with medications.
- Choose certified products. Prioritize USP, NSF, or ConsumerLab-verified brands.
- Retest after 8–12 weeks. Follow-up blood work confirms whether the supplement is working and whether the dose needs adjustment.
- Reassess regularly. Needs change with age, health status, and diet. Annual review is reasonable for most people.
Are There Alternatives to Supplement-Based Treatment?
Supplements are one tool, not the only one. Depending on the deficiency or condition, alternatives include:
- Dietary modification — Increasing intake of nutrient-dense foods (fatty fish for omega-3s, leafy greens for folate, fortified dairy for Vitamin D).
- Fortified foods — Many staple foods (cereals, plant milks, orange juice) are fortified with Vitamin D, B12, and calcium.
- Prescription medications — For severe deficiencies or conditions requiring pharmacological doses, prescription-strength formulations (e.g., Drisdol for Vitamin D, Vascepa for triglycerides) offer standardized, regulated dosing.
- Lifestyle changes — Moderate sun exposure (10–20 minutes daily without sunscreen on arms and legs) can meaningfully raise Vitamin D levels in many people.
Choose food sources if: The deficiency is mild and dietary habits are modifiable. Choose supplements if: Absorption is impaired, dietary change is not feasible, or a clinical deficiency requires faster correction.
FAQ: Using Vitamins Supplements As A Treatment
Q: Can vitamins cure diseases? A: Vitamins can treat conditions caused by deficiency (e.g., scurvy from Vitamin C deficiency, rickets from Vitamin D deficiency). They do not cure diseases with complex or unrelated causes.
Q: Is it safe to take multiple supplements at once? A: It depends on the combination. Some nutrients compete for absorption (calcium and iron, for example). Others work synergistically (Vitamin D and K2 for bone health). Always review combinations with a pharmacist or physician.
Q: Do supplements need FDA approval? A: In the United States, dietary supplements do not require FDA approval before going to market. Manufacturers are responsible for safety, but the FDA can act if a product is found to be unsafe after it’s sold.
Q: How long does it take for supplements to work? A: It varies. Iron levels may improve within 4–8 weeks; Vitamin D deficiency correction typically takes 8–12 weeks of supplementation. B12 injections can show neurological improvement over several months.
Q: Are gummy vitamins as effective as capsules or tablets? A: Gummies often contain lower doses and may lack certain nutrients (like iron) due to stability issues. They’re better than nothing but generally less reliable than capsules or tablets for therapeutic use.
Q: Can children use vitamins as a treatment? A: Yes, under medical supervision. Pediatric dosing is very different from adult dosing. Never give adult supplements to children without a clinician’s guidance.
Q: What’s the difference between a supplement and a nutraceutical? A: The terms overlap. “Nutraceutical” is a marketing term for food-derived products with health benefits. Both categories are regulated as dietary supplements in the U.S., not as drugs.
Q: Should I take supplements with food? A: Fat-soluble vitamins (A, D, E, K) are best absorbed with a meal containing fat. Most B vitamins and Vitamin C can be taken with or without food, though taking them with food reduces stomach upset.
Conclusion: Practical Next Steps
Using vitamins supplements as a treatment is grounded in real science — but only when it’s targeted, tested, and supervised. The evidence is clearest for correcting documented deficiencies and supporting specific health conditions like pregnancy, bone loss, or absorption disorders.
Actionable next steps for 2026:
- Schedule a comprehensive blood panel that includes Vitamin D, B12, folate, iron/ferritin, and magnesium if you suspect a deficiency or fall into a high-risk group.
- Bring your supplement list to your next medical appointment — including doses and brands — so your provider can check for interactions.
- Choose only third-party certified products (USP, NSF International, or ConsumerLab verified) to ensure label accuracy.
- Set a calendar reminder to retest key nutrient levels every 6–12 months if you’re on ongoing supplementation.
- Prioritize food sources first where practical, and use supplements to fill genuine gaps rather than replace a varied diet.
Supplements are a legitimate part of modern healthcare when used with evidence and intention. The key is treating them with the same seriousness as any other medical intervention.
References
- World Health Organization. (2023). Micronutrient deficiencies. https://www.who.int/health-topics/micronutrients
- National Institutes of Health, Office of Dietary Supplements. (2023). Vitamin D fact sheet for health professionals. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- National Institutes of Health, Office of Dietary Supplements. (2023). Vitamin B6 fact sheet for health professionals. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional/
- ConsumerLab. (2023). Product review: Multivitamins and supplements. https://www.consumerlab.com
- U.S. Food and Drug Administration. (2022). Dietary supplements: What you need to know. https://www.fda.gov/food/buy-store-serve-safe-food/dietary-supplements
Leave a Reply